Get in touch!
We don't provide our services to anyone else, and we are always available to help when you need us. To contact us, please fill out the following form.
Scoliosis is a three dimensional spinal deformity, involving a lateral (sideways) curvature of the spine, involving at least three vertebrae with abnormal spinal rotation. This often presents itself in asymmetrical posture and occasionally, but not always, discomfort. Scoliotic posture can present as one shoulder visibly lower than the other, protruding ribs, the shoulder blades or pelvis jutting out on one side, and a ‘skin crease’ beneath the rib cage on one side of the body.
Between 0.3- 0.5 % of the UK’s child population have scoliosis, and most types of scoliosis are more common in females than in males.
Scoliosis can have many different causes, the cause is linked intrinsically to the type of scoliosis your child has. There are four main types of scoliosis:
80% of scoliosis in children is Idiopathic Scoliosis. The term idiopathic suggests that the cause is unknown as there is no obvious cause (no bony deformity or accompanying underlying condition), however recent scientific studies have shown the cause to be genetic in origin.
Idiopathic scoliosis is further categorised according to the age of onset:
Infantile - under 3 years old
Juvenile - ages 3 to 10
Adolescent - ages 10 to 18
Adolescent Idiopathic Scoliosis is the most common type of all cases of idiopathic scoliosis, with 80% of all idiopathic cases appearing in this age category.
Congenital Scoliosis accounts for around 10% of scoliosis in children. Congenital Scoliosis is caused by a bony abnormality of the spine which is present from birth, this can be a misshapen vertebrae or vertebrae fusing together. Commonly, but not always, there is a history of scoliosis or back pain in the family.
There are occasions where congenital scoliosis can be identified in a child's infancy, however it is most commonly identified in early teenage years when the child’s body goes through the major growth spurts associated with puberty.
Neuromuscular Scoliosis accounts for between 5 and 7% of scoliosis in children and is scoliosis that becomes present as a result of a pre-existing neurological or neuromuscular condition.
The scoliosis curves in this type of scoliosis form as the result of dysfunctional nervous (Neuropathic) or muscular (Myopathic) systems. These systems in non affected individuals hold the spine in a straight and stable posture, but the dysfunction in affected individuals allows the spine to develop a curve as the body is less able to hold itself up against the pull of gravity.
Please note that this is not an exhaustive list, but some conditions that can cause Neuromuscular Scoliosis are:
Roughly 3% of scoliosis is caused by other means, this can be scoliosis caused by spinal trauma, scoliosis that develops post surgically, or scoliosis related to spinal tumours.
You may have heard some healthcare professionals talk about your child’s curvature in terms of degrees or angle, they are referring to your Child's Cobb angle. Cobb angles are the measurable degrees of your child’s curve size and often contribute to the classification of your child’s scoliosis. For more information on Cobb angles and how they are measured please click HERE.
When classifying scoliosis they take into consideration the location and apex of the curve, rotation of the spine, rib angulature and skeletal maturity through an x-ray of the pelvis or hand. The Cobb angle is also measured and taken into account, and all of these factors together will allow your child’s scoliosis to be classified.
Once the curve has been classified, this will decide how we design the brace and indicate which specific scoliosis physiotherapy exercises will be most appropriate.
If left untreated, the asymmetrical loading and pressures on your child’s spine will lead to further deformity.
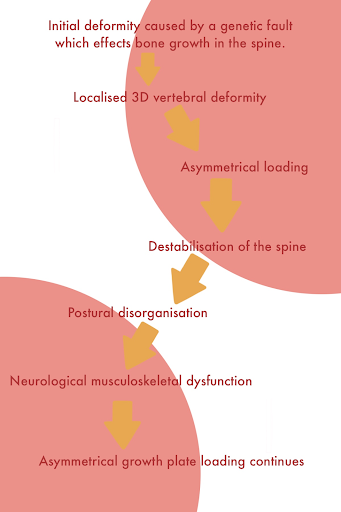
Scoliosis starts off with an initial anomaly in the vertebrae caused by a genetic fault, this can be because of a mis-matching of ossification (the fusing of bone) on one side, which leads to a localised deformity in the spinal column, as one side continues to grow after the other side has stopped. This anomaly can also be something your child is born with, like a vertebrae that has not formed correctly in the womb. Either way, this irregularity in the bones has a knock on effect.
This initial deformity means that the weight of your child’s spine and head is then carried asymmetrically - putting strain on the growth plates and aggravating the curvature caused by that initial deformity. This destabilises the spine and causes biomechanically disorganised posture, encouraging that deformity to get bigger over time.
As this is happening, the body's neurological and muscular system adapts to take on this new posture, and new neural-pathways form that reinforce and exacerbate this poor carriage of the body and continue the asymmetrical loading of the growth plates. This creates a scenario where the curvature worsens because of the loading on the spine, and the loading on the spine increases because of the curvature.
The severity of this deformity if left untreated would be dependent on how severe your child’s scoliosis is in the first place, but if left to its own devices the scoliosis will cause further damage to the spine. Bracing plays an important factor in counteracting the forces going through the spine, disrupting this cycle of continuous asymmetrical loading and minimising the impact on the spine.
No, here at Children's Orthotics we are happy to be your first port of call when you think your child may have Scoliosis. We will be able to tell you if it is likely that your child has scoliosis, and refer you to one of our experienced third party specialist spinal consultants. They will be able to confirm a scoliosis diagnosis through a series of x-rays and calculations - we will then work with this spinal consultant to give your child the care they need.
Getting your child booked in for an assessment with Children’s Orthotics is the first step in accessing our fantastic scoliosis services. At your child’s assessment appointment our orthotist will accurately assess your child’s condition to establish the correct treatment for your child’s needs. They will achieve this by performing a postural assessment, and reviewing any recent X rays taken of your child’s spine. This assessment will also involve discussing your child’s symptoms, lifestyle and goals to ensure that they are getting the best treatment for them and their lifestyle.
To get in touch or arrange an appointment, you can call us at 0330 088 3949 or email office@orthotics.co.uk.